1. Questions
In Canada, the COVID-19 pandemic has altered commuting through teleworking/remote learning, unemployment, reduced transit service, and commuter safety concerns. Previous analyses have examined mobility and traffic data (e.g. Amberber et al. 2021) to document declining transport movement. Declining public transit ridership and revenue has reduced service levels by Canadian transit agencies (Boisvert 2020). Given the potential for COVID-19 circulation across multiple years (Scudellari 2020), it is important to understand individual transport mode choices attributable to avoidance of COVID-19 risk. Using a national survey, this paper explores changes in commute mode due to COVID-19 among Canadians and the effects of coarse sociodemographic variables on this relationship, asking: what is the association between the mode of transport used before COVID-19 and changes in commute mode to avoid COVID-19 risk?
2. Methods
We examined data from the Canadian Perspectives Survey Series (CPSS) 3: Resuming Economic and Social Activities During COVID-19 (Statistics Canada 2020b). We used the CPSS3 Public Use Microdata File (PUMF), released in December, 2020. The survey was conducted by Statistics Canada in June, 2020, as part of a multi-wave effort to evaluate the impact of COVID-19 on Canadians. In June of 2020, the first wave of the pandemic had waned in most parts of Canada and many sectors had begun reopening (Canadian Institute for Health Information 2020). The CPSS3 targeted Canadians 15 years and older, excluding residents of Northern Territories. Persons living on-reserve, in institutions, and in “extremely remote” areas were also excluded. We followed Statistics Canada guidelines regarding the use of survey weights to construct percentage estimates and minimum raw counts for denominators of proportions (Statistics Canada 2020a). Any unweighted Ns provided below have been rounded to the nearest 100 to comply with guidelines (Statistics Canada 2020a).
Of the 4,200 total participants in the CPSS3, we analyzed a subset (n~2900, representing 23,069,500 Canadians) who were “pre-COVID-19 commuters”: those who indicated a mode of transport in response to “What was your main mode of transportation to work or school prior to the COVID-19 pandemic?” We compared the indicated modes to the “current mode of” to observe changes in mode share.
To examine avoidance of COVID-19 risk, we used a question posed to respondents who indicated a change in their main mode of to work or school: “What are the reasons for the change in your main mode of ?” Participants who selected “COVID-19 risk” in response defined our key outcome (1= if commute changed with “COVID-19 risk” as the reason, 0 otherwise). We conducted logistic regression to model the odds of changing commute due to COVID-19 risk. Our primary explanatory variable was mode of transport to work or school before COVID-19. Relevant covariates available in CPSS3 were age, sex, level of education, immigration history (yes/no), and urban/rural location. Lastly, we examined percentage of current modes among for pre-COVID-19 public transit commuters (n~300). Analyses were performed using SAS 9.4 (Cary, NC, USA).
3. Findings
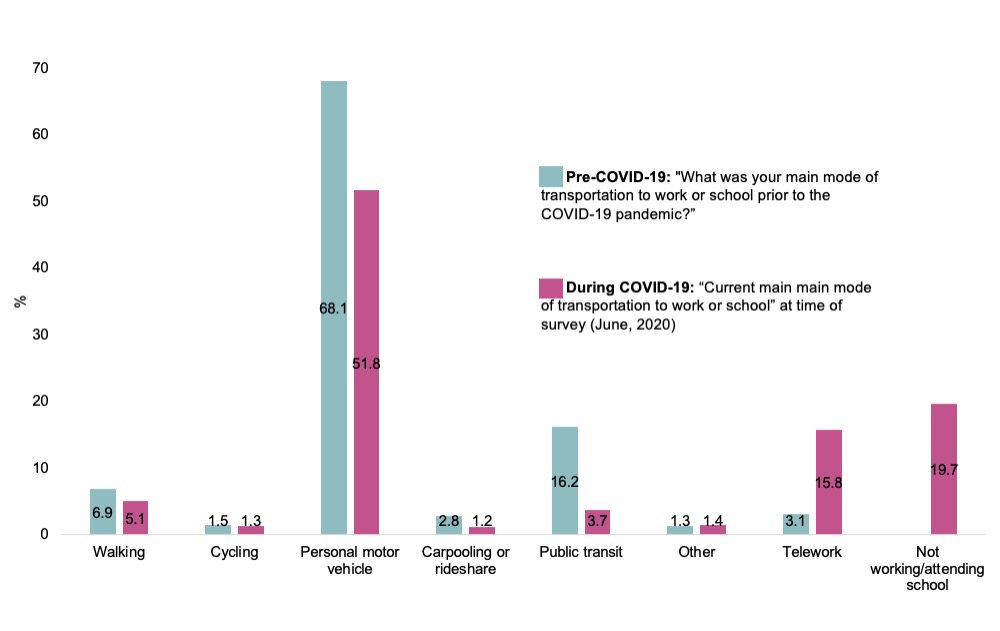
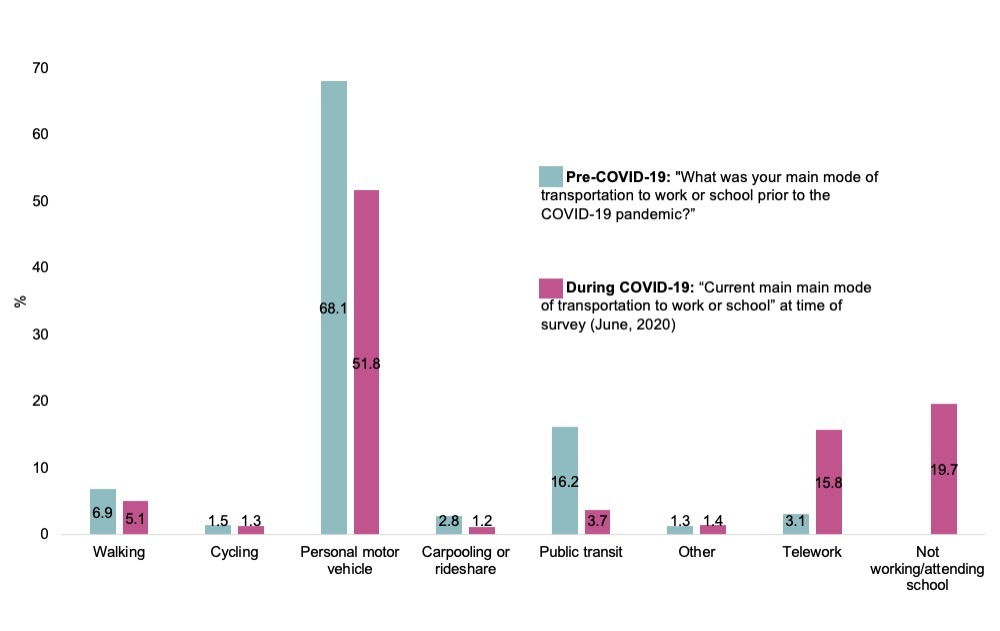
Among pre-COVID-19 commuters, 17.8% (SEadjusted: 1.3%) changed their commute mode due to COVID-19 risk. Comparing commute modes before and during COVID-19 (Figure 1), declines were observed in all out-of-home modes of transport, with increases in telework and no work/school.
Most pre-COVID-19 commuters (Table 1) had university-level education, lived in urban settings, and were born in Canada. Most used personal motor vehicles for travel to work and school before COVID-19. Among those who changed their commute due to COVID-19 risk, there were more younger people, women, urban-dwellers and those who used transit before COVID-19.
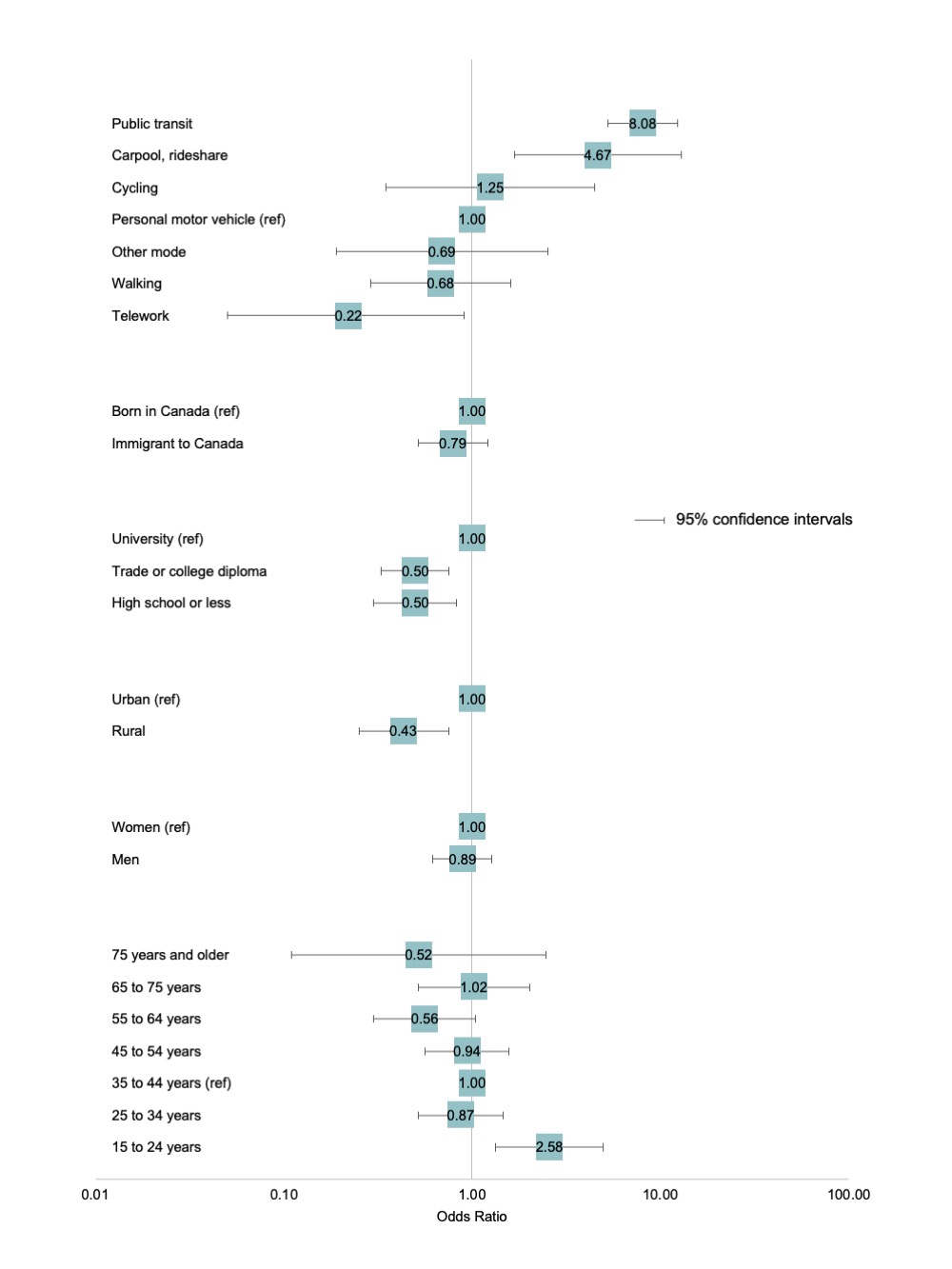
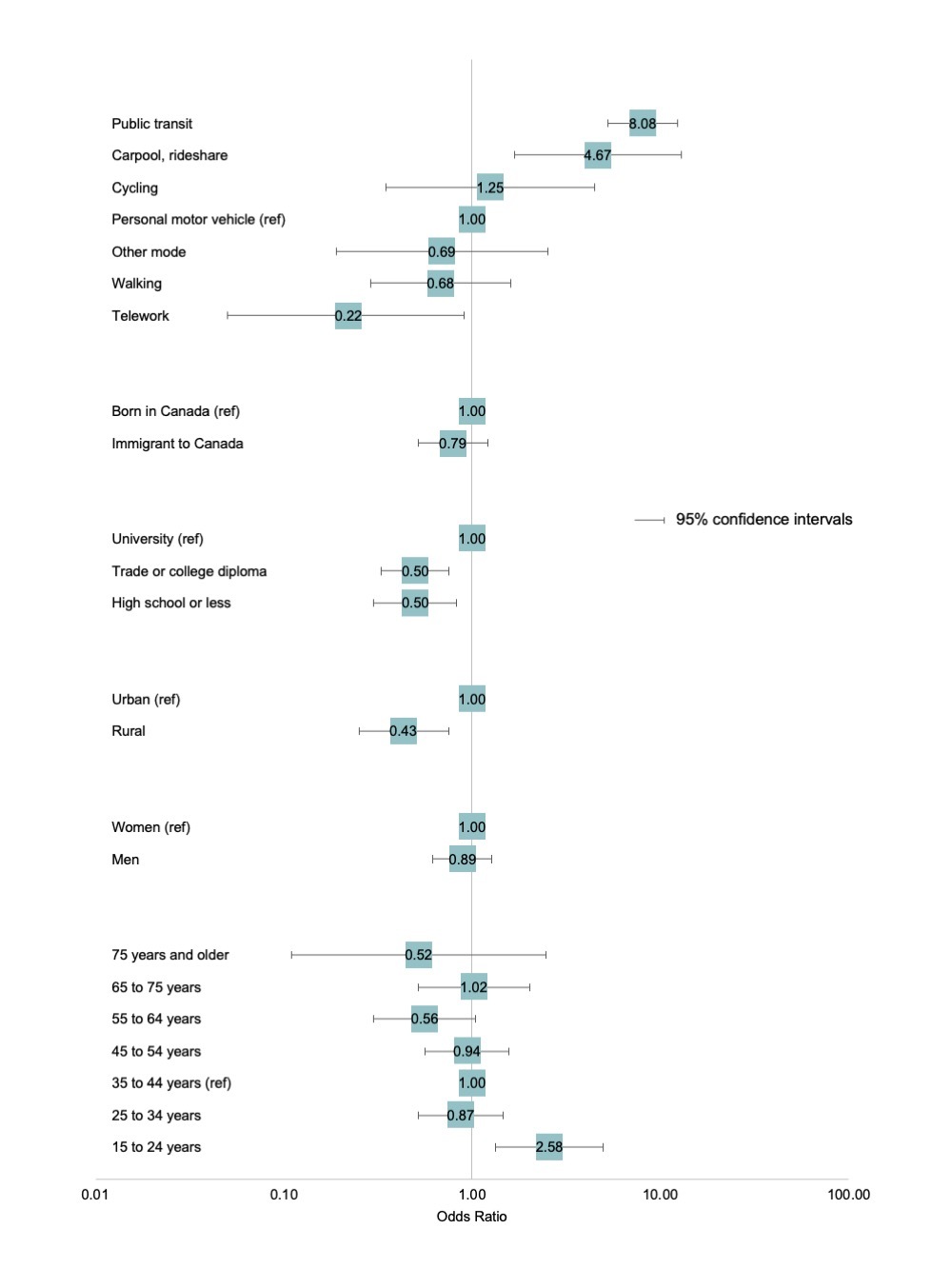
In our multiple logistic regression (Figure 2), use of public transit and carpooling/rideshare before COVID-19 had the strongest associations with the odds of commute change motivated by COVID-19 risk. Those who teleworked prior to COVID-19 had reduced odds of changing commute mode due to risk, as did those who walked, although the 95% confidence interval for this estimate included an odds ratio of 1. Among covariates, those without university education (both high school level and college and trade certificates) had lower odds of a change in commute due to COVID-19 risk, which could be attributable to high proportion of these Canadians in essential jobs that can’t be performed by telework. Rural location was also inversely associated with a change in commute due to COVID-19 risk, as compared to urban locations. We note here that the CPSS3 target population excludes many rural parts of Canada (Northern Territories and “very remote” regions), and we emphasize the need for more detailed information on rural regions, which may experience disproportionate pandemic impacts (Savage et al. 2020).
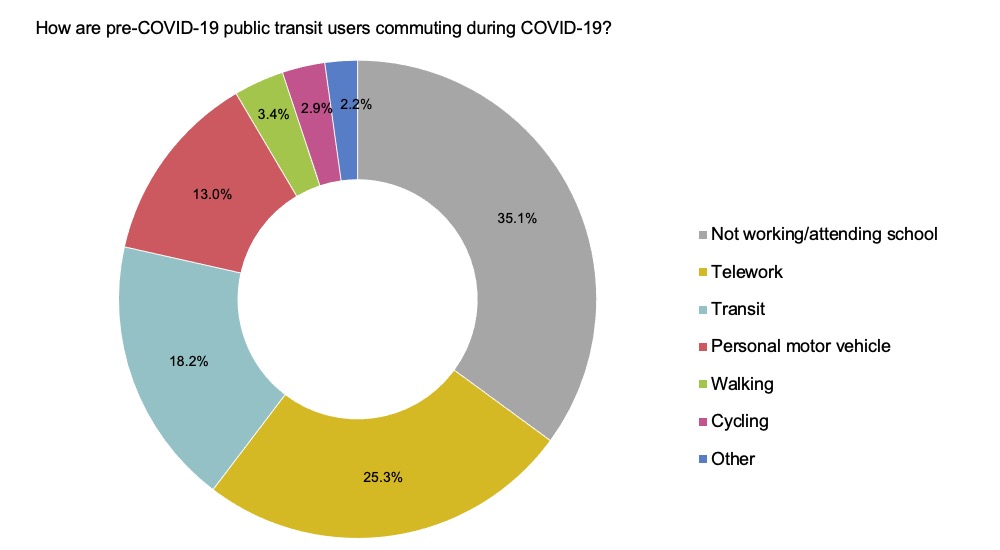
Current commute mode for pre-COVID-19 public transit users is shown in Figure 3. A plurality of these users reported currently “not attending work or school”, a composite category challenging to interpret given the absence of a student status indicator in the CPSS3. Because telework was a distinct category, “not attending work or school” comprises a mix of Canadians who left the work force during the pandemic (unemployed and retired), along with students remote learning or on break from school (if not attending work during this break). Among pre-COVID-19 public transit users still commuting at the time of survey collection, public transit remained the most used mode, but personal motor vehicle reliance was substantial among this population, and exceeded active modes of travel. While this indicates a cause for concern for both traffic management and population health in the post-pandemic recovery, regional data will be important to identifying local patterns in adoption of new travel modes. There is also a crucial need to incorporate relevant data on social determinants that the CPSS3 PUMF lacks, including ethnicity, race, occupation, and income, to ensure equitable management and recovery (McKenzie 2020).

Acknowledgements
Data for this study were collected by Statistics Canada and public use data access was provided by the Ontario Data Documentation, Extraction Service and Infrastructure (<odesi>), managed by the Ontario Council of University Libraries (OCUL). Salary support for MBC was provided by a Canadian Institutes of Health Research (CIHR) operating grant held by MAH.