1. Questions
Nearly 50 million Americans have low vision, and many encounter daily transportation barriers that hinder access to essential services, including healthcare (American Foundation for the Blind 2024; Khimani et al. 2021; Lam and Leat 2013). Scarce transportation in rural areas further limits residents’ access to care (Goldstein et al. 2012; Starbird et al. 2019).
This study investigates clinicians’ perspectives on transportation barriers to low vision care. It makes a significant contribution to the limited body of work highlighting clinicians’ viewpoints, representing an underexplored area of transportation research (Fields et al. 2020; Oluyede, Cochran, Prunkl, et al. 2022; Oluyede, Cochran, Wolfe, et al. 2022). Our work focused on clinicians in Nebraska and Kansas—both predominately rural Midwestern states. The clinicians’ extensive experience with low-vision patients from diverse backgrounds provides valuable insights into the unique challenges faced by suburban and, especially, rural populations, which remain underrepresented in prior research.
The research addressed two key questions:
-
What transportation barriers do clinicians observe among their patients seeking healthcare?
-
How do these barriers affect patients’ health and well-being?
2. Methods
Following previous research on transportation barriers to healthcare, we conducted 8, 20–30-minute, semi-structured interviews over Zoom with clinicians in Nebraska and Kansas. Qualitative techniques using open-ended interviews offer opportunities to understand “complex, multifaceted challenges,” and clinicians provide insights into financial, geographical, social, and infrastructural barriers (Ballantyne et al. 2019; Fields et al. 2020; Oluyede, Cochran, Prunkl, et al. 2022). This work employed purposive and snowball sampling of clinicians recruited through emails and phone calls using publicly available information and recommendations from other clinicians. Our sample included occupational therapists (3), optometrists (2), and ophthalmologists (3) who have worked with low-vision patients ranging from 5 to 40 years at their current locations. Due to the limited number of low vision specialists in the Midwest, our sample size reflects a substantial number of providers serving the area. We conducted interviews between October and December 2024. The Institutional Review Board at the University of Nebraska-Lincoln approved the study.
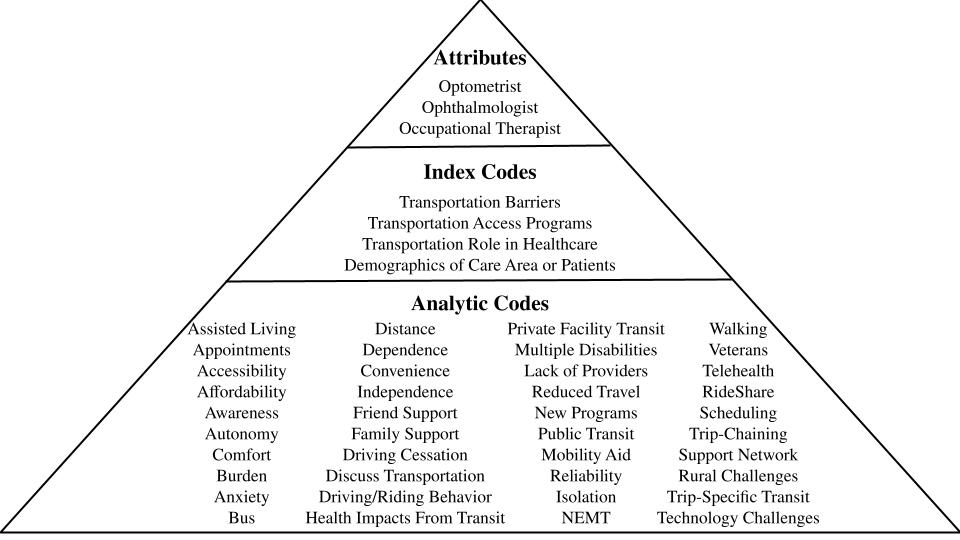
Two authors recorded, transcribed, and coded all interviews using a flexible coding approach in Dedoose, a qualitative data analysis (QDA) software. The codes (Figure 1) were applied across three hierarchical categories: attributes describing interviewee characteristics, index codes linked to interview questions, and analytic codes capturing specific themes within participants’ narratives (Deterding and Waters 2018).

3. Findings
Despite the distances that rural low-vision patients travel, appointments are frequently canceled and rescheduled for therapy and check-ups. Interviewees attributed this issue to dependence on others for transportation—typically family members, private facilities (e.g., assisted living facilities), and local transit agencies. These options can leave patients waiting at clinics for hours for a ride to pick them up (Table 1). Public transit users in urban areas may experience relatively shorter wait times compared to those relying on paratransit, private facility transportation, or family members for travel. Occupational therapists and previous research noted that the care provided to individuals facing transportation barriers is negatively impacted when appointments are delayed or missed (Oluyede, Cochran, Prunkl, et al. 2022).
Clinicians mentioned individuals with low vision rely heavily on their support networks, such as family or friends, for transportation. These friends and family members assist with medical and non-medical activities, leading to greater dependence among individuals with low vision. This dependence often carries feelings of being a burden, which clinicians observed (Table 1). This reliance is usually inconsistent or unreliable, as patients must navigate others’ schedules without a guaranteed ride. Individuals with low vision often face driving cessation later in life, making transitioning to alternative transportation a significant challenge (Cochran 2020). Beyond transportation, many older adults, with and without disabilities, struggle with technology—including telehealth platforms and ride-hailing applications—further complicating access to healthcare. Occupational therapists noted that patients wanted to improve their technology skills to increase their confidence and independence.
Clinicians providing low vision care are sparse and overburdened, especially in rural areas. As a result, some patients must travel 3–6 hours for a single visit, relying on private cars because rural public transportation is limited or unavailable (Table 1). Patients unwilling to ask family or friends for such long rides may forego care entirely, as noted by an optometrist who saw patients stop coming to appointments when they no longer felt comfortable asking their family members for a ride. These trips can impose significant financial burdens on families, as perceived by the interviewees. Furthermore, smaller populations in rural areas are often unaware of resources available for individuals with low vision. For example, when someone in a family loses their vision, there is limited awareness within the community about how to seek help or access support, which was noted by an ophthalmologist working with blind and low-vision children.
Clinicians expressed concerns about the transportation challenges reported by their patients, citing reliability and affordability as significant issues. Unreliable public transit and costly ride-shares were frequently mentioned (Table 1). To address these concerns, Omaha, Nebraska, has implemented a “Share A Fare” program which provides a 50% refund for ride-share services for individuals with low vision. In Kansas City, occupational therapists visit patients in their homes within a 60-mile radius of the clinic. One clinician shared that her sister, who has a disability, lives in San Francisco and has access to inexpensive transit from the city. Rural towns and clinics can model programs like home visits and transport subsidies to better serve populations with low vision and other disabilities. This presents an aspirational model for Nebraska, Kansas, and beyond that prioritizes accessible and equitable transportation for individuals with disabilities, enabling reliable access to healthcare without reliance on private vehicles.
Acknowledgments
The U.S. Department of Transportation supported this research financially through the University of Nebraska-Lincoln (UNL) Mid-America Transportation Center for Transportation Safety and Equity under contract number 69A3552348307. UNL’s Research Council: Faculty Seed Grants program also supported this research.