1. Questions
People in the United States spend nearly 90% of their time indoors, most commonly at home, and yet we know little about how heat health outcomes vary by housing type and tenure (Gabbe, Mallen, and Varni 2022; Klepeis et al. 2001). Indoor temperatures are affected by structure design, air conditioning access, and the ability to afford energy costs (Iverson et al. 2020; Ostro et al. 2010; Stone et al. 2021). People with low-incomes and people of color experience broad thermal inequities, but these have been largely studied at neighborhood scales and outside of the housing context (Jesdale, Morello-Frosch, and Cushing 2013; Mitchell and Chakraborty 2018; O’Neill, Zanobetti, and Schwartz 2005). We answer the question: How are housing and household characteristics associated with heat-related health risk?
2. Methods
We used the Residential Energy Consumption Survey (RECS), a nationwide household survey conducted by the U.S. Energy Information Administration (EIA). The Public Use Microdata for 2020 includes 18,496 respondents and provides a representative sample of U.S. occupied housing units (U.S. EIA 2020). The survey’s heat health-related questions measure the frequency that a home was kept at an unhealthy temperature and whether someone in the household needed medical attention because the home was too hot. Although we do not know if respondents’ unhealthy temperature reports refer to hot or cold, there is likely a large overlap given research about household energy insecurity.
We first summarized the two heat risk variables by housing type, tenure, race, ethnicity, and income using survey weights provided by the U.S. EIA (U.S. EIA 2020). We then specified two sets of logistic regression models with households as the unit of analysis. Our binary outcome variables were: (1) kept home at an unhealthy temperature; and (2) needed medical attention due to a hot home. Independent variables pertained to housing type, tenure, setting, other housing characteristics, and household characteristics. These categories and variables are listed in the left two columns of Table 2. Additional details about model variables are included in this paper’s Supplemental Information. Models 1 and 3 only include housing type and tenure variables and models 2 and 4 include all independent variables.
3. Findings
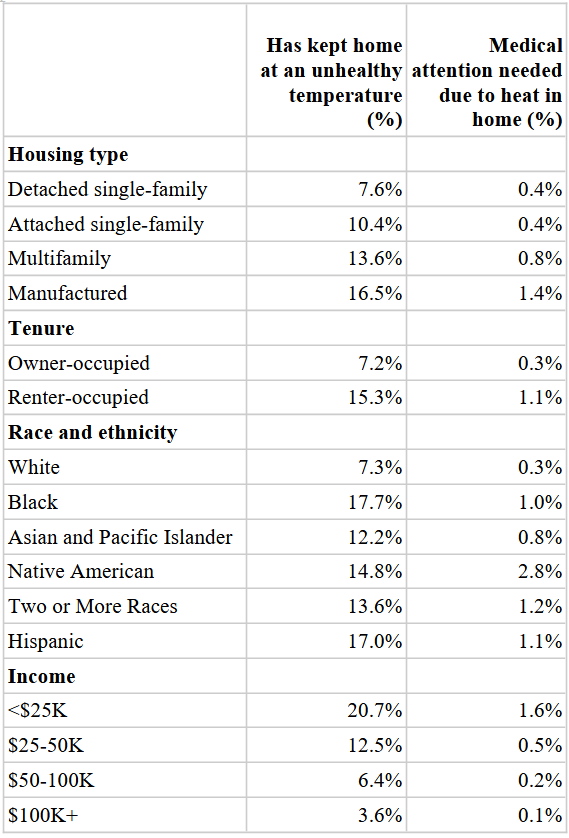
Households in manufactured and multifamily housing – and renter households in general – face the greatest health-related risks (Table 1). The differences are considerable when comparing manufactured housing and multifamily with detached single-family residences. Manufactured housing residents are more than twice as likely (16.5% vs. 7.6%) as detached single-family residents to keep their home at an unhealthy temperature and are nearly four times likelier to need medical attention due to heat in the home (1.4% vs. 0.4%). Renter-occupied households are more than twice as likely (15.3% vs. 7.2%) to keep their homes at an unhealthy temperature and more than three times likelier (1.1% vs. 0.3%) to need medical attention due to heat in the home.

Heat-related health disparities are much worse for Black, Native American, Hispanic, and multiracial households compared with white households, and to a lesser extent Asian and Pacific Islander, households. For example, Black, Native American, and Hispanic households are at least twice as likely to keep their homes at an unhealthy temperature relative to white households. The disparities are particularly pronounced in terms of seeking heat-related medical attention. Native American households are about nine times likelier (2.8% vs. 0.3%) and Hispanic households are more than three times likelier (1.1% vs. 0.3%) than white households to seek medical attention.
Low-income households also experience greater heat disparities. More than 20% of households with incomes below $25K keep their homes at an unhealthy temperature and 1.6% seek medical attention compared with 3.6% and 0.1% respectively of households with incomes of at least $100K.
The regression results indicate some disparities by housing type and tenure, even after controlling for household characteristics (Table 2). Manufactured housing residents are more likely to keep their homes at unhealthy temperatures (models 1 and 3) but these relationships are not statistically significant after controlling for other factors (models 2 and 4). Renters are positively associated with heat risk across all models, though the coefficients shrink after controlling for other factors.
Other housing characteristics are also associated with heat risk. Households with window AC or no AC are more likely to keep their home at an unhealthy temperature than households with central AC. Households that experienced broken AC equipment in the previous year are much more likely to have unhealthy home temperatures or need heat-related medical attention. Households that reported adequate insulation are less likely to have homes at unhealthy temperatures or need medical attention.
Households headed by a person of color and low-income households face greater heat risk. Black, Asian and Pacific Islander, other race (which includes Native American and multiracial households), and Hispanic households are all more likely to keep their homes at unhealthy temperatures. Households in the other race category are also more likely to need medical attention, while the three other race/ethnicity categories are not significantly different than white households. Households with incomes below $50K per year – roughly 200% of the poverty line for a family of four – are considerably more likely to keep their homes at an unhealthy temperature and need heat-related medical attention.
Two other household characteristics are positively connected with heat risk. Larger households are positively associated with unhealthy temperatures. In keeping with the literature, senior households are less likely to keep their home at an unhealthy temperature but need heat-related medical attention more often.
These findings underline the importance of identifying and mitigating disparities in thermal health. This study echoes previous research about thermal inequities by race, ethnicity, and economic status. Additionally, we show that unhealthy temperatures and heat-related medical attention are more prevalent for renters, even after controlling for race and income. Scholars have an opportunity to better understand the housing-related mechanisms related to heat health, and policy makers should target renters and manufactured housing residents for interventions.
Acknowledgements
This research was supported by a Santa Clara University Sustainability Research Grant. We thank the attendees of the 2022 Association of Collegiate Schools of Planning conference for their useful feedback.